The Advisory Council on Alzheimer’s Research, Care, and Services presented updates on Alzheimer Disease (AD) and AD and related dementias (ADRD) treatments and ongoing AD research in a virtual meeting held in January.
Representatives from the National Alzheimer Project Act (NAPA) research committee, Washington University School of Medicine (WashU), and the Alzheimer’s Association reported on the developments in disease modifying therapies (DMTs), funding, resources for dementia caregivers, and the connection between AD and Down syndrome.1
DMTs for AD
From 2016 to 2023, researchers have observed advancements in AD treatment. Most recently, the US Food and Drug Administration (FDA) approved Leqembi (lecanemab), an amyloid beta-targeting antibody for patients with AD and those in the mild cognitive impairment (MCI) or mild dementia stage of the disease. The FDA’s decision on donanemab, also an amyloid beta-targeting antibody, for the treatment of patients with early AD, is anticipated in the first quarter of 2024.
The approved route of administration for lecanemab is intravenous (IV). Eisai Pharmaceuticals is testing a subcutaneous route of administration. Compared with the IV route, initial reports suggest that subcutaneous formulations clear 14% more plaque, have an 11% higher area under the curve (AUC), and have lower systemic injection reaction rates.2
On January 31, 2024, Biogen Inc. decided to discontinue Aduhelm (aducanumab-avwa) production, sales, and the affiliated clinical study. Instead, they will allocate their resources to the development of other treatment methods for AD and prioritize moving forward with lecanemab.3
Growing Resources for Dementia Caregivers
With recent progress in AD treatments, progress has also been made in the availability of resources for dementia caregivers. The Alzheimer's Association collaborated with the Centers for Disease Control and Prevention (CDC), Building Our Largest Dementia (BOLD) Public Health Center of Excellence on Dementia Caregiving, and Emory University to initiate a free interactive public health curriculum for clinicians, students, and educators. The goal is to increase awareness and knowledge about the importance of dementia caregiving and how public health may affect it.
Representatives of the advisory board addressed further initiatives concerning racial/ethnic diversity needs between patients and caregivers and demanded an increase in caregiver wage. Although a resolution has not been reached, caregiving networks are optimistic to find ways to implement changes in the near future.4
"
The research and the investments that have been made over the past decades led to these advancements in understanding the disease, how it starts and progresses, and figuring out ways to intervene in it.
Revisions and Updates to Funding AD Research
Various extensions and reauthorizations have been made to continue AD research. There is bipartisan agreement that AD research needs more attention. The National Institutes of Health (NIH) and the CDC are looking to:
Extend and reauthorize NAPA
Continue advising the Centers for Medicare and Medicaid Services (CMS) to implement a dementia care management model
In the senate budget requests for the 2024 fiscal year, the NIH requested a $321 million increase and the CDC requested $35 million for the BOLD infrastructure for the Alzheimer Act. The Act focuses on AD diagnosis, treatment, and dementia caregiving.5
Increases in federal funding have advanced AD research and the progression of clinical trials. “It’s research that changes the cookbook of medicine ... The research and the investments that have been made over the past decades led to these advancements in understanding the disease, how it starts and progresses, and figuring out ways to intervene in it,” Randall Bateman, MD, Charlotte and Paul Hagemann distinguished professor of neurology at WashU in St. Louis, said at the meeting.6
Researchers at WashU have identified challenges that have limited treatment objectives.7
Overall Barriers to AD Research
Racial & Ethnic Disparity
- Racial and ethnic groups are excluded from testing - Overall lack of research about patients with AD who belong to racial and ethnic groups
Accessibility to Infusion Centers
- Patients who live in rural areas have difficulty accessing infusion centers - Infusion treatments are time consuming. Patients often miss due to vacation, travel, and other illnesses. - 6–8-month waitlist for treatment - Small window for treatment
Cost of treatment
- Treatment costs $50,000 per year - Medicare finances only 80% of treatment expenses, which could leave patients with ~$10,000 bill out of pocket - AD biomarker testing is not offered insurance coverage
Effectiveness of DMTs
- Need for precision medicine for an individual's unique disease profile - Dosage and duration vary per patient - Some patients need to switch medications
Although limitations are presented in the infrastructure for AD/ADRD treatment, the researchers highlight initiatives for AD prevention. These include the early administration of lecanemab and the implementation of the combination of DMTs.8
The Connection Between AD and Down Syndrome
In highlighting the existing challenges with AD treatments, Elizabeth Head, MA, PhD, professor at the University of California, spoke about the connection between AD and Down syndrome (DS). By age 40, patients with DS have sufficient plaque and tangle pathology for an AD diagnosis. Dr Head mentioned that it is widespread for older patients with DS to develop AD, and it is one of the leading causes of death for this patient population.
Though there is a connection between AD and DS, patients with DS are often excluded from AD trials, presenting a barrier in research. Ultimately, there is a lack of racial and ethnic diversity in trials; only White patients have a higher survival rate.
Since there is still a limited amount of evidence, it is difficult to identify pharmacologic intervention effectiveness for cognitive decline in patients with DS. Dr Head urged that researchers should begin to expand AD studies to this patient population. The inclusion of patients with DS in cohort trials would result in advanced AD research and a better understanding of DS.9
Dementia is a worldwide public health concern. There are 35.6 million people worldwide with dementia; by 2030, estimates are that 75.6 million people worldwide will have dementia.Dementia prevalence doubles every 5 years after age 65, and by age 90, nearly 1 in 3 adults will meet the diagnostic criteria for dementia.1
Hallmarks of aging include chronic low-grade inflammation, mitochondrial dysfunction, and neurodegenerative changes. The concept of “inflammaging," introduced in 2000 by Claudio Franceschi, correlates aging with elevated inflammatory markers, which make older individuals more susceptible to chronic morbidities, including Alzheimer disease (AD).2 Oxidative stress and mitochondrial dysfunction in AD perpetuate an imbalance in neuronal cell function, generating further malfunction. In AD, brain atrophy and reduction in cerebral perfusion are significant, with a yearly hippocampal volume reduction of 3.5% in people with mild cognitive impairment compared with 1% to 2% in healthy controls aged 55 and older.3,4 Cerebral blood flow is decreased up to 40% in patients with AD compared to healthy controls.5
Cardiorespiratory fitness, as measure by VO2max (volume of oxygen per kilo of body weight per minute) is affected by age, gender, genetics, exercise type, and training intensity. After age 20, it is estimated that VO2max decreases by 3% to 6% each decade, with a jump to more than 20% decline per decade after age 70.6 Several studies correlate higher VO2max with lower inflammation, reduced oxidative stress, improved mitochondrial function, and improvement in brain structure and functional connectivity.5,6,7
Effective treatments for Alzheimer disease (AD) are lacking, which is shifting the focus to disease prevention. While the benefits of exercise are frequently noted, reported measurements of physical fitness are inconsistent across studies, and many participants self-report their physical activity. Recommended guidelines for exercise are also vague. Considering the effects of cardiorespiratory fitness on inflammation, mitochondrial structure, and cerebral anatomical changes will aid in providing future recommendations for dementia prevention, including AD, and overall cognitive health.
Cellular Aging and Inflammation as a Cause of Dementia
A number of cellular changes are associated with chronic low-grade inflammation and impairment in immune function. Shrinking of the thymus is one of the most dramatic changes that occurs in an aging immune system. Naïve T-cells leave the thymus to circulate in the blood and lymphatic system to protect against pathogens. Memory T-cells form after antigen exposure. With age, T-cells develop underlying defects and decline in activity, contributing to chronic inflammation and decreased immunity. Naïve T-cell production (CD4 and CD8) also declines with age, and memory T-cell production increases. In older individuals, memory CD4 T-cells show impaired mitochondrial function and increased production of reactive oxygen species.8 During chronic inflammation associated with age, pro-inflammatory cytokines, such as interleukin (IL)-6, tumor necrosis factor (TNF), and IL-1β, cross the blood-brain barrier, triggering microglia and astrocytes to produce pro-inflammatory cytokines over anti-inflammatory cytokines.9
Increased dementia risk is noted with comorbid neuropsychiatric and cardiovascular conditions and high systemic inflammation. Apolipoprotein E gene variant APOEε4 is the strongest genetic risk factor for dementia. APOEε4 is also linked to atherosclerosis and the modulation of inflammatory cytokines through promoting innate immune response.10 Beeri et al noted that having 2 or more cardiovascular risk factors in midlife predicted an increase in amyloid aggregation later in life.11 The researchers noted that midlife risk factors outweigh late-life risk factors in the development of dementia. Gottesman et al found that 2 or more cardiovascular risk factors (BMI ≥30, smoking, hypertension, diabetes, hypercholesterolemia) in midlife had an odds ratio of 2.88 for later-life brain amyloid deposition.12 This is important to note since the neurodegenerative changes of dementia begin decades before clinical symptoms are evident.
Neuroinflammation is evident in the progression of AD through increasing amyloid plaques and neurofibrillary tangles (NFTs).13 Overactivation of the immune response is more pronounced in AD because of the accumulation of amyloidβ protein (Aβ).5 So-called proteinopathies, which occur due to misfolding of toxic proteins, produce extracellular Aβ plaques and intracellular NFTs. When amyloid beta precursor protein (APP) is cleaved by gamma-secretase, an Aβ-peptide forms containing 42 amino acids, known as Aβ42, which is the most toxic variant.9 In addition to tau and phosphor-tau, Aβ42 is a biomarker for AD that can be measured in cerebrospinal fluid via lumbar puncture.9 The accumulation of pathologic Aβ42 in the AD brain is attributed in part to impaired mitophagy.14
The presence of Aβ plaques contributes to the hyperphosphorylation of tau. The functioning of tau, the major microtubule-associated protein in neurons, is regulated by its degree of phosphorylation. Increased tau phosphorylation decreases microtubule stability and is correlated with neurotoxicity. In AD, tau is noted to be 3 to 4 times more phosphorylated, accounting for the increased formation of NFTs.14
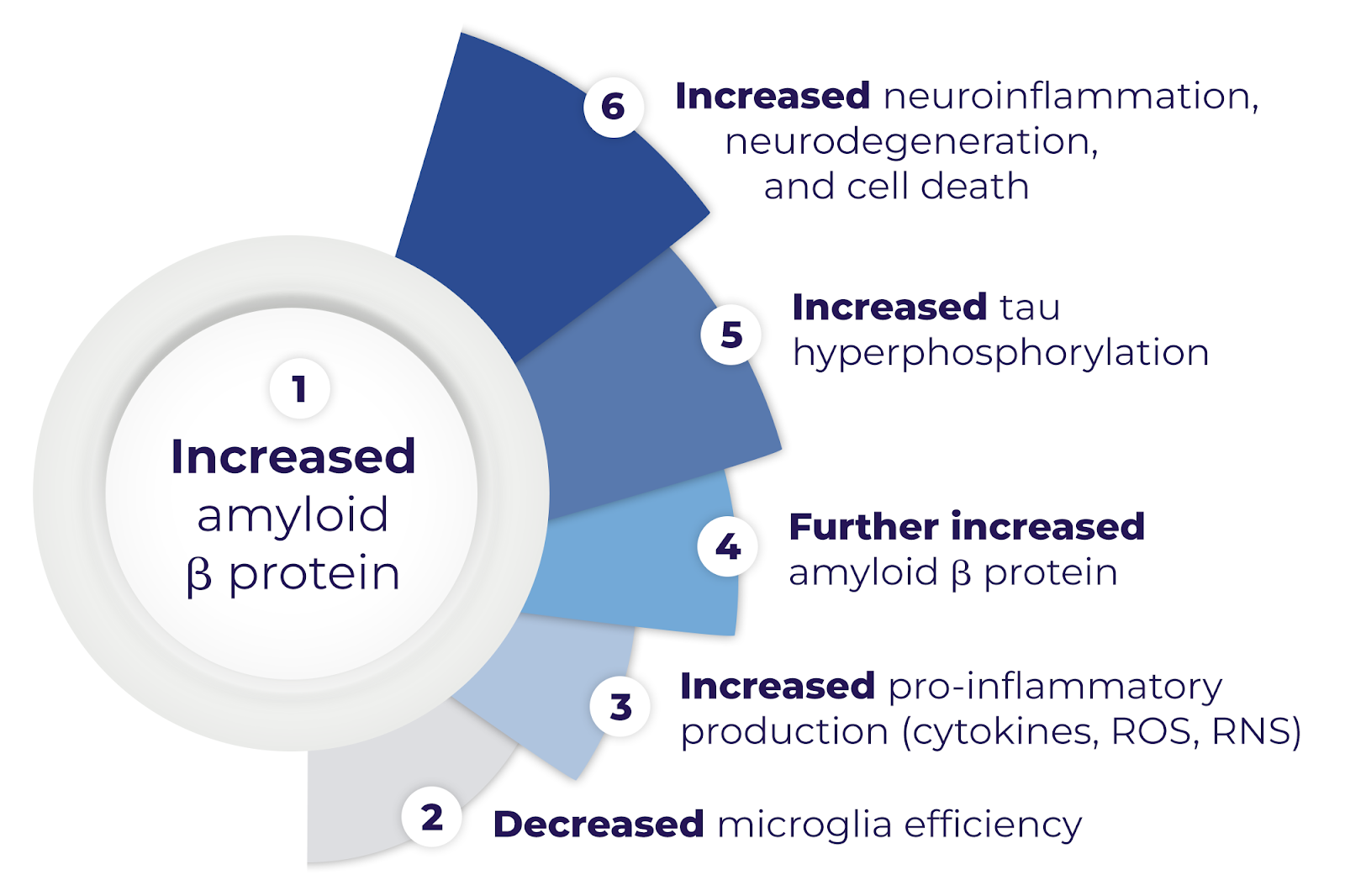
In aging, prolonged immune activation causes impairment of phagocytosis by microglia and degradation of astrocytes.5 An essential role for microglia and macrophages in the central nervous system is to discard cellular debris, while astrocytes aid neuronal stability by modulating the blood-brain barrier.5 The phagocytic role of microglia in the central nervous system to degrade Aβ is compromised, which leads to the release of pro-inflammatory products. As a result, inflammatory cytokines, including ILIβ and TNF-α, pass the blood-brain barrier. Proinflammatory production of cytokines, reactive oxygen, and reactive nitrogen species furthers the production of Aβ and tau hyperphosphorylation through a positive feedback loop leading to more toxicity, as shown in Figure 1.5
Figure 1. Progression of amyloid β protein causes microglia inefficiency, and produces pro-inflammatory species (cytokines, reactive oxygen species [ROS], reactive nitrogen species [RNS]), causing further amyloid β production, and tau hyperphosphorylation, ultimately leading to neurodegeneration and cell death.
Effects of Exercise on Inflammation
Over the past 3 decades, several studies have correlated decreased inflammation with decreased AD risk. The Baltimore Longitudinal Study of Aging showed a 60% reduction in dementia in patients using NSAIDs for over 2 years. Zhang et al found a 19% risk reduction in AD with NSAID use from 16 cohort studies.15
Lack of physical activity is associated with elevated inflammatory biomarkers. For example, abdominal adipose tissue secretes TNF-α and other inflammatory markers.16 Conversely, physical activity increases hormones with immunomodulatory effects, increases anti-inflammatory myokines, decreases visceral fat, and decreases expression of toll-like receptors in immune cells.17 Exercise enhances immunocompetence by circulating immune cells to peripheral tissue. A study by Lavin et al showed that lifelong exercisers had significantly lower levels of IL-6 and higher levels of anti-inflammatory markers IL-10, TNF-α, TNF-β, and EP4.18 Repeated moderate intensity exercise is shown to have antioxidative effects, decrease oxidative stress, improve mitochondrial efficiency, and improve the immune function response.18 All of these factors result in a cumulative reduction in inflammation.
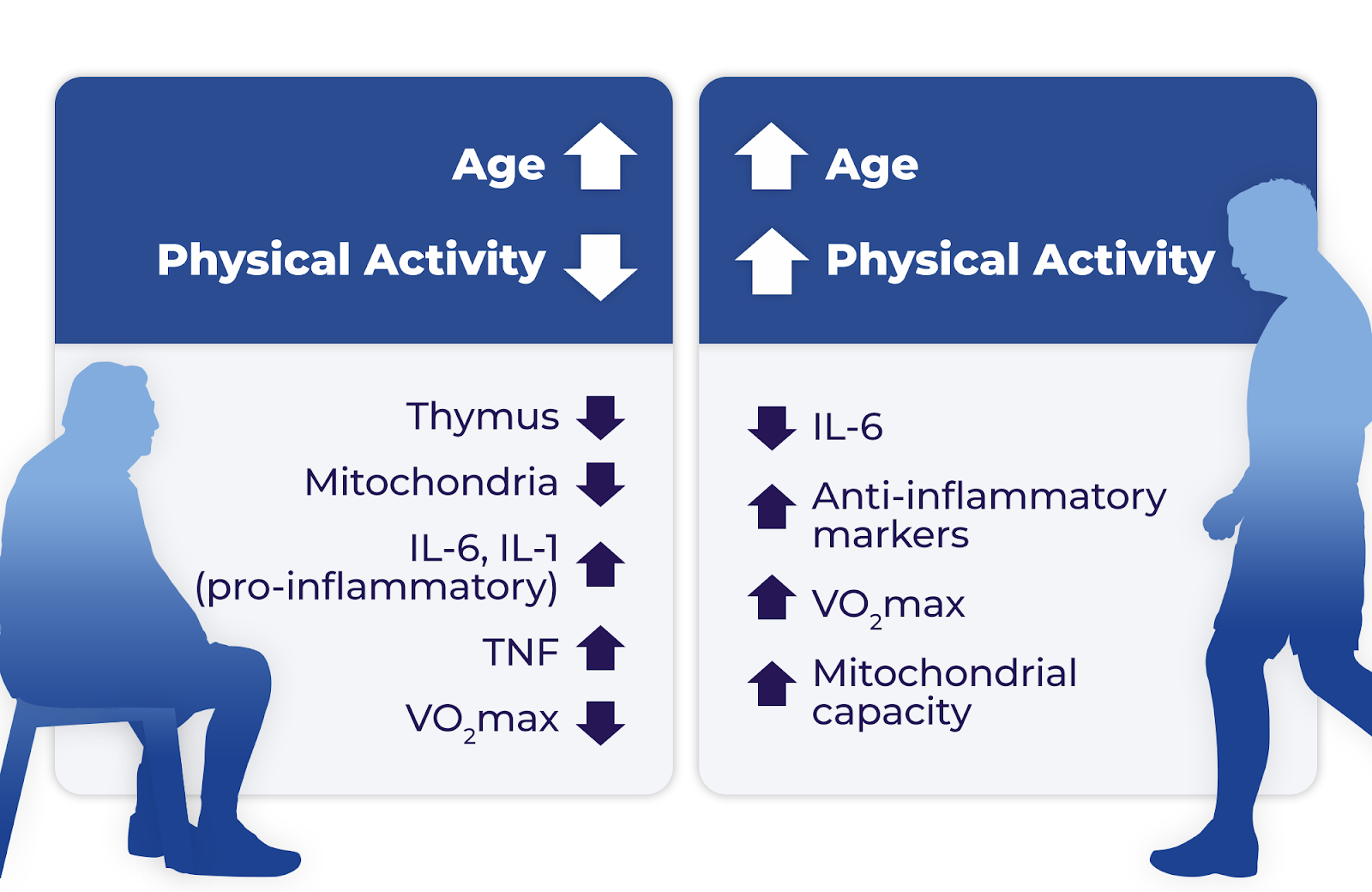
Dougherty et al studied 86 older adults at risk for AD, comparing cardiorespiratory fitness, hippocampal volume measured by magnetic resonance imaging (MRI), and memory measured by Rey Auditory Verbal Learning Test (RAVLT).19 The results differed based on gender, showing that VO2max was associated with increased hippocampal volume in women and improved RAVLT memory scores in men. Increased age and decreased physical activity correlate with impaired thymus function, impaired mitochondrial function, decreased VO2max, and increased inflammatory markers IL-6 and IL-1. An increase in physical activity in advancing age is associated with a reduction in IL-6 and increases in anti-inflammatory markers, VO2max, and mitochondrial capacity (Figure 2).19
Mitochondria generates adenosine triphosphate (ATP) through oxidative phosphorylation. Additionally, calcium homeostasis, apoptosis, and reactive oxygen species (ROS) production are mitochondrial functions. The accumulation of amyloid β peptide within mitochondria is associated with the progression of AD; study findings show amyloid-β protein precursor and Aβ in mitochondria in AD patients before the formation of senile plaques.20
Mitochondria use oxygen to produce energy during metabolism. If ROS levels are unusually elevated, neurodegeneration occurs through the oxidation of proteins that causes damage to their structure. The ROS levels are regulated by mitophagy, a process by which damaged organelles are engulfed by vesicles and degraded by specialized proteins. With aging, the decreased efficiency of antioxidants and the increase in ROS cause toxicity, leading to cellular dysfunction and apoptosis.21
Postmortem brain studies of individuals with AD show that mitochondrial dysfunction occurs early in the disease process and is especially pronounced in the entorhinal-hippocampal system located in the medial temporal lobe. Cortical neurons in the entorhinal-hippocampal system layer II are thought to be where initial AD pathology occurs.14 Postmortem studies have also shown a decrease in the number and quality of mitochondrial DNA (mtDNA).20
Mitochondrial biogenesis, the creation of new, functioning mitochondria, is thought to be facilitated by physical activity.22 In 1965, the research of John O. Holloszy, MD, showed that endurance exercise training resulted in the doubling of mitochondria in rodent skeletal muscle. Endurance exercise training improves mitochondrial capacity, which enables protective antioxidant effects.22 He noted that mitochondrial biogenesis occurs with repeated bouts of exercise at sufficient intensities over a period of time.
Ding et al reported that regular exercise caused increased mitochondrial tricarboxylic acid enzymes and the synthesis of neurotrophins, including brain-derived neurotrophic factor (BDNF).23 BDNF is a mediator in PGC-1α-induced mitochondrial biogenesis and regulates antioxidant enzymes that reduce ROS seen in AD.A positive correlation between mitochondrial volume and VO2max has been noted since the 1970s.24 While VO2max is typically used to measure cardiorespiratory fitness, it depends on mitochondrial efficiency.23 In addition to mitochondria volume, endurance exercise and higher VO2max are associated with improvement in mitochondria respiratory function and oxidative capacity.24
More recent research has replicated the effect of exercise on mitochondria in other organs, notably the brain. The brain utilizes 20% of the body's total oxygen and depends on mitochondria for 90% of its ATP production.20 Radak et al reported that endurance exercise increases VO2max and is associated with mitochondrial biogenesis partly through sirtuins (SIRT-3), a mitochondrial protein. SIRT-3 is responsible for oxidative phosphorylation, oxidation of fatty acids, and synthesis of ketone bodies.Endurance exercise increases SIRT-3 levels in the hippocampus, skeletal muscle, liver, and heart.25
Effects of Exercise on Brain Structure and Cerebral Blood Flow
General cerebral atrophy is a well-known occurrence with aging, and hallmarks of this include volume loss, cortical thinning, enlarged ventricles, and brain folding changes. Global volume changes begin at age 35 with a total brain volume loss yearly of 0.2%, which escalates to 0.5% annually after age 60.26 The hippocampus and prefrontal cortex appear more vulnerable to aging; the hippocampus and prefrontal cortex atrophy by 1% to 2% for every year after age 55.3 Cortical thinning occurs at a rate of 0.004 mm/year and is associated with memory decline. Ventricular enlargement occurs from the accumulation of cerebrospinal fluid in the ventricles, which causes compression of brain parenchyma. Specifically, the lateral and third ventricles are associated with impaired attention, visual memory, and speed.26 A study comparing middle-aged adults with healthy older individuals noted that sulci were, on average, 17.3% wider in elderly patients (aged 66-90 years).26 Of note, the most significant difference between the middle age and elderly adults was in the depth of the left superior frontal sulcus.26 A larger longitudinal study with 132 participants followed over a 7 year period found the largest rate of increase in fold opening in the superior frontal sulcus (0.131 mm/year). Like other neurodegenerative diseases, AD accelerates and intensifies structural changes that occur with aging.26
Vascular changes that occur with age include arterial stiffness, reduced capillary density, and increased blood-brain barrier permeability.26 Decreased cerebral blood flow is associated with increased dementia risk, and is noted prior to structural brain changes in AD. Reduced cerebral blood flow has been predictive of progression to AD from healthy controls and individuals with mild cognitive impairment.27
Exercise is correlated with increased hippocampal volume, hippocampal neuroplasticity28, increased gray matter volume28, white matter integrity3,, and cortical thickness.24 A 1-year study of 120 participants aged 55 to 80 found that moderate-intensity aerobic training showed a 2% increase in anterior hippocampal volume.29 Conversely, a study by Pani et al showed increased hippocampal atrophy in high-intensity interval training groups, and that brain structure was best preserved in those following the national guidelines of 30 minutes of physical activity per day. This study also noted that those with higher VO2max at inclusion had better-preserved brain structure.30 A study of 29 participants with mild cognitive impairment by Eisenstein et al correlated increased VO2max with reduced hippocampal volume. However, there was a decreased correlation between hippocampal volume and memory performance compared with low VO2max.4 Alfini et al determined that cessation of exercise for 10 days reduced hippocampal blood flow.7
Regular exercise and a higher VO2max in mid-life seem to have the most robust evidence for ameliorating cognitive changes that occur with age. A study by Kurl et al followed over 2000 men over 20 years and found that one standard-deviation increase in VO2max (3.5 mL/kg/min) correlated with a 20% decrease in dementia.29 Men with a VO2max less than 23.7 mL/kg/min (low cardiac fitness) had a 1.92-fold risk of developing dementia compared with those with a VO2max greater than 36.5 mL/kg/min at baseline testing.29 Horder et al followed 1462 women and reported a 9.5-year delay in dementia onset in more fit women in midlife.30
While these studies looked at how various exercise regimes influence VO2max, brain structure, and cognition, the most beneficial exercise program seems to be moderate-intensity cardiovascular exercise, performed consistently 5 to 6 days a week, and starting by mid-life. VO2max improves with repeated sessions of physical activity of at least 30 minutes that elevates the heart rate, such as brisk walking, jogging, biking or hiking. Although some studies indicate cognitive gains with single bouts of exercise, longer term studies highlight the importance of cardiorespiratory fitness starting in mid-life. Higher V02max at age 50 correlates with delaying dementia onset by a decade.30 Midlife cardiovascular risk factors (including BMI ≥30, smoking, hypertension, diabetes, hypercholesterolemia) are associated with elevated dementia risk later in life.12 Since exercise is known to improve cardiovascular risk factors, it seems likely that it should also reduce dementia risk. More research is needed in this area and to evaluate the effects of other forms of exercise, such as weight training or yoga, on cognitive decline.
Conclusion
AD is typically an age-related disease occurring later in life, with an increased risk associated with cardiovascular disease, diabetes, and obesity. As people continue to live longer, and the age of the world's population increases, dementia is also increasing.
Inflammation is a known by-product of aging and exercise reduces inflammation. While reports of the impact of exercise on memory are conflicting, most show at least modest improvement in one or more aspects of cognition. Studies have shown that as little as a single exercise session can cause changes in the body.
Measurement of cardiorespiratory fitness utilizing VO2max is a way to standardize studies of physical fitness. Limitations include self-reported exercise and a minimal number of participants. As more studies are done, specific recommendations for VO2max levels will help individuals quantify their fitness goals to maximize their cognitive health.
Cynthia Sieto, MSPAS, DMSc, graduated with her MSPAS from DeSales University in 2001 and her DMSc from Rocky Mountain University in 2023. She has specialized in psychiatry for 20 years and is currently employed by St. Luke’s University Health Network in Allentown, PA. To maximize her cardiorespiratory fitness, she completed the 2023 NYC marathon.
"
["post_title"]=>
string(121) "Does Increased Cardiorespiratory Fitness Decrease Alzheimer’s Risk? The Impact of Physical Fitness on Neurodegeneration"
["post_excerpt"]=>
string(109) "Exercise is likely to slow the onset and progression of brain changes and dementia due to Alzheimer disease.
"
["post_status"]=>
string(7) "publish"
["comment_status"]=>
string(6) "closed"
["ping_status"]=>
string(6) "closed"
["post_password"]=>
string(0) ""
["post_name"]=>
string(45) "cardiorespiratory-fitness-decrease-alzheimers"
["to_ping"]=>
string(0) ""
["pinged"]=>
string(0) ""
["post_modified"]=>
string(19) "2023-12-08 09:18:12"
["post_modified_gmt"]=>
string(19) "2023-12-08 14:18:12"
["post_content_filtered"]=>
string(0) ""
["post_parent"]=>
int(0)
["guid"]=>
string(42) "https://www.neurologyadvisor.com/?p=124676"
["menu_order"]=>
int(0)
["post_type"]=>
string(4) "post"
["post_mime_type"]=>
string(0) ""
["comment_count"]=>
string(1) "0"
["filter"]=>
string(3) "raw"
}
[2]=>
object(WP_Post)#5312 (24) {
["ID"]=>
int(121697)
["post_author"]=>
string(5) "45391"
["post_date"]=>
string(19) "2023-09-22 09:38:06"
["post_date_gmt"]=>
string(19) "2023-09-22 13:38:06"
["post_content"]=>
string(12293) "
Alzheimer disease (AD) is a devastating neurodegenerative disorder. In the United States, approximately 6.5 million people aged 65 years and older are living with AD and nearly two-thirds of them are women.1 It can have particularly devastating ripple effects on caregivers; in 2021, more than 11 million unpaid caregivers provided nearly 16 billion hours of care valued at $271.6 billion to individuals with AD.1
With no known cure for AD, many studies are examining preventative measures, such as the use of estrogen hormone therapy (EHT). Because estrogen facilitates cognitive function and declines during menopause,2 researchers have investigated a possible causal relationship between estrogen deficiency and the onset of AD. Natural menopause is defined as 12 consecutive months of unintentional amenorrhea and has an average age of onset of 51 years.2 Perimenopause describes the time leading up to menopause.2 For most other hormone-deficient diseases, such as hypothyroidism, the treatment is hormone replacement.
When administered during menopause, EHT could improve cognitive function and potentially prevent the development of AD. This timing is important. The risks and benefits of postmenopausal EHT have been a controversial topic since the Women’s Health Initiative (WHI) study was stopped prematurely due to the incidence of breast cancer and cardiovascular disease.3 Unfortunately, because the publication was based on incomplete statistics, many of the findings of this study were presented as more substantial than the actual data support.4
Many of the risks associated with EHT reported in the Women’s Health Initiative (WHI) study are not seen if therapy is started early in menopause. In addition, the WHI study only evaluated synthetic conjugated equine estrogens,3 and participants were up to 15 years postmenopausal, therefore they were without pre-menopausal levels of estrogen and progesterone for a long enough period of time to develop cardiovascular disease and osteoporosis, for example.4 In recent studies, EHT started near the onset of menopause and/or at age 60 years or younger was safe and decreased all-cause mortality.5 This timeframe presents an opportunity to possibly prevent age-related cognitive decline in women.6
Alzheimer Disease
Epidemiology
As noted, AD disproportionately affects women. Because AD pathology precedes clinical manifestations by decades, this higher risk cannot be accounted for by the longer lifespan of women compared with men.6 Early-onset AD, which occurs before age 65, is rare and has been associated with an autosomal dominant inheritance pattern. In people aged 65 years and older, AD is the fifth-leading cause of death.1 From 2000 to 2019, the mortality rate for AD increased by more than 145%, while the number of deaths from heart disease and stroke decreased.1
Pathophysiology
The exact etiology of AD is unknown. Certain risk factors have been identified, such as advancing age, female sex, and a first-degree relative who has had AD.1 The presence of the e4 form of the apolipoprotein E (APOE-e4) gene has been associated with an increased risk for AD.1 Recent studies have also suggested an inflammatory pathway in AD, which might be triggered by chronic fungal, bacterial, or viral infections.7
Physiologic changes in the brain that occur with AD include atrophy and abnormal deposition of beta-amyloid and tau proteins.1 Beta-amyloid protein forms clumps outside the neurons (plaques), and tau protein forms clumps inside the neurons (neurofibrillary tangles).1 These changes cause devastating neuronal dysfunction that manifests clinically as memory loss, progressive cognitive decline, and ultimately, death.1
Diagnosis
The diagnosis of AD is made via a detailed clinical assessment of the patient, including cognitive function, after alternative diagnoses have been excluded. Abnormal levels of beta-amyloid and tau proteins can be identified in cerebrospinal fluid and by positron emission tomography imaging,1 however, these studies are not routinely done due to their invasiveness and cost. A definitive diagnosis of AD can be made post-mortem at autopsy by identifying the hallmark brain changes of plaques and neurofibrillary tangles.
Estrogen
Role in Cognitive Function
The vast estrogen receptor network in the brain controls brain energy metabolism and many other systems.6 Estradiol, the most physiologically important type of estrogen,2 enhances brain function in several ways such as by improving neuronal growth and protecting neurons from injury.8 Several brain areas that are essential for memory and learning, such as the prefrontal cortex and amygdala, have a significant number of estrogen receptors and rely on estrogen availability for proper functioning.6
Deficiency
During perimenopause, estrogen levels fluctuate unpredictably; in menopause, they decline steadily. When estradiol levels decrease, fundamental cellular changes occur in the brain. These include reductions in dendritic spines, synaptic density, and the number of synapses present.2 The regulation of brain glucose metabolism by estrogen dissipates, creating a hypometabolic state.6 These physiologic changes result in “brain fog” characterized by poor concentration and memory problems.9 Although these transformations typically reverse with menopause,9 they illustrate the undesirable effects of estrogen deficiency on cognition. The duration of time without estrogen also matters. Studies have shown that a woman who enters surgical menopause at a younger age has a higher rate of cognitive decline and AD-related pathology.2
Estrogen Hormone Therapy
Cognitive Benefits
The beneficial effects of EHT on the brain have been well documented. Boyle et al described increased gray and white matter volume in women who had a history of oral estrogen use, including synthetic conjugated equine estrogens, as measured using structural magnetic resonance imaging.10 The Cache County Study found that women using EHT had a decreased incidence of AD compared with those who did not use EHT, and the longest use of EHT (>10 years) reduced the risk for AD the most.11
In contrast, other studies have shown that EHT does not decrease the risk for AD. For example, no cognitive benefits were observed in patients taking EHT despite neuroimaging results showing reductions in both biomarkers for brain aging and the deposition of the beta-amyloid protein.9 In addition, although patients with the APOE-e4 gene are at increased risk for AD, one study suggests that this population has the fastest cognitive decline when taking EHT.9
Timing
Many pathologic changes that occur with AD begin years before the patient develops clinical symptoms.2 Therefore, if EHT is considered, it should be initiated well before the onset of cognitive decline. Studies have suggested that the most beneficial time to start EHT is at or near the onset of menopause.6 EHT also has protective effects against cardiovascular disease when started during this timeframe.12
Considerations
Despite the relationship between estrogen and cognitive function, data for the role of EHT in neuroprotection are inconclusive.9 Currently, the American College of Obstetricians and Gynecologists and the North American Menopause Society do not support its use as primary prevention of cognitive dysfunction,13,14 and the International Menopause Society guidelines cite a lack of evidence to support this use.15 One of the limitations of previous studies, such as the landmark WHI Memory Study,16 is that they included postmenopausal women older than 65 years of age. The studies also did not consider the window of opportunity to begin estrogen replacement at or near the onset of menopause. Further research is needed to explore the potential benefits of administering estrogen during this time frame.
Risks
The decision to start EHT should be individualized for each patient. Hormone therapy should be avoided in those with contraindications, such as a history of estrogen-dependent cancer, thromboembolic events, or a blood clotting disorder. A progestin or progesterone should be given with estrogen if the patient has not had a hysterectomy, as unopposed estrogen can cause endometrial hyperplasia and potentially endometrial cancer.14
Conclusion
Alzheimer disease has a greater incidence in women; therefore, research studies have focused on the beneficial role of estrogen in cognition and the potential of EHT to prevent AD. Some evidence suggests that a window of opportunity exists for EHT initiation at or near the onset of menopause when this therapy is safe and could have neuroprotective effects. Further research is needed to determine factors such as efficacy, dosing, route of administration, and duration of treatment.
At the Alzheimer’s Association International Conference 2023, several studies on the use of blood tests for the diagnosis and treatment of Alzheimer disease (AD) were presented, highlighting the viability of blood tests for future AD screening.
Currently, there are barriers when it comes to the use of blood tests for AD such as; requiring patients to visit a specialized clinic and have the test administered by trained personnel, with time-limited temperature-dependent delivery and storage procedures.
Finger Prick Test Detects Blood-Based Biomarkers of AD
Capillary blood collected through finger prick was as reliable as blood collected through standard venous method in detecting AD biomarkers. Furthermore, the blood samples were stably transported within 1 day with no specific storage conditions.
In a pilot study,1 researchers collected blood from 77 patients from a memory clinic through finger prick and standard venous blood collection. The finger-pricked blood samples were transferred onto capillary dry blood spot cards, while the venous blood samples were transferred onto venous dry blood spot cards. The dry blood spot cards were then shipped overnight without temperature control or cooling.
Researchers compared plasma biomarkers related to AD — neurofilament light, glial fibrillary acidic protein, and phosphorylated tau (p-tau181 and p-tau217) — in the capillary and venous dry blood spots to EDTA plasma.
"
Blood tests for Alzheimer’s disease have great potential for improving diagnostic accuracy and proper treatment of people with Alzheimer’s.
The levels of glial fibrillary acidic protein (r= 0.7180; P <.0001), neurofilament light (r= 0.6967; P <.0001), and p-tau217 (r=0.8995; P =.0002) found in the capillary dry blood spots significantly correlated with their respective levels in EDTA plasma. Only p-tau181 levels from the capillary dry blood spots did not correlate with the same levels in EDTA plasma. The venous dry blood spots were also found to have similar detectable biomarker levels as EDTA plasma.
AD Blood Tests May Improve Diagnostic Accuracy in Primary Care
Blood tests accurately detected AD in more than 75% of cases, while physicians correctly identified AD in 54% of cases, highlighting the viability of blood tests for improving diagnostic accuracy in a primary care setting.
For the BioFINDER-Primary Care study,2 researchers examined 307 patients (mean age, 76 years; 48% women; 49% AD pathology) who had cognitive complaints. They aimed to compare the diagnostic accuracy of blood plasma-collected p-tau217 ratio and Aβ42/40 ratio with standard diagnosis by primary care physicians (PCPs). The PCPs were assigned to diagnose AD based on the results from computerized tomography (CT) scans, magnetic resonance imaging (MRI) scans, and cognitive tests. Their diagnosis was compared to the findings of C2N’s Precivity AD2 blood test, which utilizes mass-spectrometry to measure the p-tau217 ratio and Aβ42/40 ratio, which are blood plasma biomarkers of AD.
AD pathology was confirmed by the US Food and Drug Administration (FDA)-approved cerebrospinal fluid Aβ42/p-tau181 test or readings of 18F-flutemetamol from an amyloid-β positron emission tomography scan.
The researchers found that the Precivity AD2 blood test had decent accuracy; the area under the curve (AUC) was 0.80 (95% CI, 0.75-0.86) for the Aβ42/40 ratio, 0.91 (95% CI, 0.88-0.94) for the p-tau217 ratio, and 0.94 (95% CI, 0.92-0.97) for the algorithm.
Additionally, in those with available PCP questionnaires (n=265), the PCPs were able to correctly diagnose AD in 54% of the cases, while the Aβ42/40 ratio and p-tau217 ratio correctly identified 77% and 85% of patients, respectively.3
A total of 87% of PCPs followed treatment guidelines, but that led to 50% of confirmed patients with AD that did not receive symptomatic treatment and 30% of patients who did not have AD incorrectly received symptomatic treatment. The physicians’ mean certainty of diagnosis for AD was recorded as 4.7 out of 10.
AlzoSure Predict Test Has High Predictive Ability for AD
A blood test was found to predict cognitive deterioration due to AD within 2 years and 6 years with an AUC of almost 1, which indicates perfect accuracy. This further demonstrates how blood tests can be used in patients at risk for AD.
Using data from the Australia Imaging, Biomarkers and Lifestyle study,3 researchers collected blood samples from 479 individuals with and without cognitive impairment aged 60 to 85. The researchers used this data to assess the ability of Diadem US Inc’s AlzoSure Predict blood test to accurately determine whether individuals aged older than 50 will experience significant cognitive decline due to AD years before the full onset of symptoms. Accuracy was measured via AUC; an AUC of 0.5 signifies 50% accuracy while an AUC of 1 represents perfect accuracy.
The blood test predicted cognitive deterioration due to AD within 2 years and 6 years with an AUC of 99.8% and 98.4%, respectively.
“Due to the lack of accurate diagnostic tools, it is currently very difficult for primary care doctors to identify Alzheimer’s disease… Blood tests for Alzheimer’s disease have great potential for improving diagnostic accuracy and proper treatment of people with Alzheimer’s,” said the researchers, in a press release.4